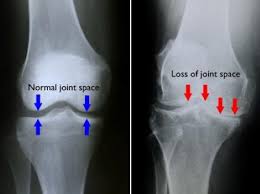
Osteoarthritis of the knee (knee OA) is the inflammation and wearing away of the cartilage on the bones that form the knee joint (osteo=bone, arthro=joint, itis=inflammation). The diagnosis of knee OA is based on 2 primary findings: radiographic evidence of changes in bone health (through medical images such as X-ray and magnetic resonance imaging [MRI]), and an individual’s symptoms (how you feel). Approximately 14 million people in the United States have symptomatic knee OA. Although more common in older adults, 2 million of the 14 million people with symptomatic knee OA were younger than 45 when diagnosed, and more than half were younger than 65.
What is Osteoarthritis of Knee?
Knee osteoarthritis (knee OA) is a progressive disease caused by inflammation and degeneration of the knee joint that worsens over time. It affects the entire joint, including bone, cartilage, ligaments, and muscles. Its progression is influenced by age, body mass index (BMI), bone structure, genetics, muscular strength, and activity level. Knee OA also may develop as a secondary condition following a traumatic knee injury. Depending on the stage of the disease and whether there are associated injuries or conditions, knee OA can be managed with physical therapy. More severe or advanced cases may require surgery.
How Does it Feel?
Individuals who develop knee OA may experience a wide range of symptoms and limitations based on the progression of the disease. Pain occurs when the cartilage covering the bones of the knee joint wears down. Areas where the cartilage is worn down or damaged exposes the underlying bone. The exposure of the bone allows increased stress and compression to the cartilage, and at times bone-on-bone contact during movement, which can cause pain. Because the knee is a weight-bearing joint, your activity level, and the type and duration of your activities usually have a direct impact on your symptoms. Symptoms may be worse with weight-bearing activity, such as walking while carrying a heavy object.
Symptoms of knee OA may include:
Worsening pain during or following activity, particularly with walking, climbing, or descending stairs, or moving from a sitting to standing position
Pain or stiffness after sitting with the knee bent or straight for a prolonged period of time
A feeling of popping, cracking, or grinding when moving the knee
Swelling following activity
Tenderness to touch along the knee joint
Typically these symptoms do not occur suddenly or all at once, but instead develop gradually over time. Sometimes individuals do not recognize they have osteoarthritis because they cannot remember a specific time or injury that caused their symptoms. If you have had worsening knee pain for several months that is not responding to rest or a change in activity, it is best to seek the advice of a medical provider.
How Is It Diagnosed?
Knee OA is diagnosed by 2 primary processes. The first is based on your report of your symptoms and a clinical examination. Your physical therapist will ask you questions about your medical history and activity. The therapist will perform a physical exam to measure your knee's movement (range of motion), strength, mobility, and flexibility. You might also be asked to perform various movements to see if they increase or decrease the pain you are experiencing.
The second tool used to diagnose knee OA is diagnostic imaging. Your physical therapist may refer you to a physician, who will order X-rays of the knee in a variety of positions to check for damage to the bone and cartilage of your knee joint. If more severe joint damage is suspected, an MRI may be ordered to look more closely at the overall status of the joint and surrounding tissues. Blood tests also may be ordered to help rule out other conditions that can cause symptoms similar to knee OA.
How Can a Physical Therapist Help?
Once you have received a diagnosis of knee OA, your physical therapist will design an individualized treatment program specific to the exact nature of your condition and your goals. Your treatment program may include:
Range-of-motion exercises. Abnormal motion of the knee joint can lead to a worsening of OA symptoms when there is additional stress on the joint. Your physical therapist will assess your knee’s range of motion compared with expected normal motion and the motion of the knee on your uninvolved leg. Your range-of-motion exercises will focus on improving your ability to bend and straighten your knee, as well as improve your flexibility to allow for increased motion.
Muscle strengthening. Strengthening the muscles around your knee will be an essential part of your rehabilitation program. Individuals with knee OA who adhere to strengthening programs have been shown to have less pain and an improved overall quality of life. There are several factors that influence the health of a joint: the quality of the cartilage that lines the bones, the tissue within and around the joints, and the associated muscles. Due to the wear and tear on cartilage associated with knee OA, maintaining strength in the muscles near the joint is crucial to preserve joint health. For example, as the muscles along the front and back of your thigh (quadriceps and hamstrings) cross the knee joint, they help control the motion and forces that are applied to the bones.
Strengthening the hip and core muscles also can help balance the amount of force on the knee joint, particularly during walking or running. The “core” refers to the muscles of the abdomen, low back, and pelvis. A strong core will increase stability throughout your body as you move your arms and legs. Your physical therapist will assess these different muscle groups, compare the strength in each limb, and prescribe specific exercises to target your areas of weakness.
Manual therapy. Physical therapists are trained in manual (hands-on) therapy. Your physical therapist will gently move your muscles and joints to improve their motion, flexibility, and strength. These techniques can target areas that are difficult to treat on your own. The addition of manual therapy techniques to exercise plans has been shown to decrease pain and increase function in people with knee OA.
Bracing. Compressive sleeves placed around the knee may help reduce pain and swelling. Devices such as realignment and off-loading braces are used to modify the forces placed on the knee. These braces can help "unload" certain areas of your knee and move contact to less painful areas of the joint during weight-bearing activities. Depending on your symptoms and impairments, your physical therapist will help determine which brace may be best for you.
Activity recommendations. Physical therapists are trained to understand how to prescribe exercises to individuals with injuries or pain. Since knee OA is a progressive disease, it is important to develop a specific plan to perform enough activity to address the problem, while avoiding excessive stress on the knee joint. Activity must be prescribed and monitored based on the type, frequency, duration, and intensity of your condition, with adequate time allotted for rest and recovery. Research has shown that individuals with knee OA who walked more steps per day were less likely to develop functional problems in the future. Your physical therapist will consider the stage and extent of your knee OA and prescribe an individualized exercise program to address your needs and maximize the function of your knee.
Modalities. Your physical therapist may recommend therapeutic modalities, such as ice and heat, to aid in pain management.
If Surgery Is Required
The meniscus (the shock absorber of the knee) may be involved in some cases of knee OA. In the past, surgery (arthroscopy) to repair or remove parts or all of this cartilage was common. Current research, however, has shown that—in a group of patients who were deemed surgical candidates for knee OA with involvement of the meniscus—60% to 70% of those who first participated in a physical therapy program did not go on to have surgery. One year later, those results were unchanged. This study suggests that physical therapy may be an effective alternative for people with knee OA, who would prefer to avoid surgery.
Sometimes, however, surgical intervention, such as arthroscopy or a total knee replacement, may be recommended. There are many factors to consider when determining the appropriate surgical treatment, including the nature of your condition, your age, activity level, and overall health. Your physical therapist will refer you to an orthopedic surgeon to discuss your surgical options.
Should you choose to have surgery, your physical therapist can assist you prior to and following your surgery. The treatment you require following surgery will depend on a variety of factors such as the type of surgery performed, your level of function, and fitness prior to surgery. Contrary to popular belief, surgery is not the easy choice; you will still require treatment following your surgery to maximize your level of function.
Can this Injury or Condition be Prevented?
Many conditions, including knee OA, can be prevented with the right fitness and exercise program. Physical therapists are experts in movement. Some ways that a physical therapist can help you prevent knee OA include:
Developing an appropriate exercise program. Inactivity is a significant contributor to many problems that affect individuals, including knee OA. Strengthening the muscles around the knee, as well as surrounding joints, can help decrease stress to the knee joint. Exercises to improve flexibility can help you maintain motion in the knee joint, which helps keep the cartilage healthy. Your physical therapist can design an individualized treatment program to boost your strength and flexibility, based on your specific condition.
Weight loss. Excessive weight can increase stress to the knee joint, which in turn can contribute to the wearing away of the protective cartilage, leading to knee OA. Your physical therapist can assess your weight, perform testing to determine your fitness level, establish an exercise program, and recommend lifestyle changes. The therapist also may refer you to another health care provider, such as a dietician, for further guidance.
Activity modification. Individuals often move or perform activities in a way that is unhealthy or inefficient, or that places excessive stress on the body, including the knee joint. Your physical therapist can teach you better ways to move in order to ease stress on your body and your knees.
Taking a “whole body” approach to movement. Lack of strength, mobility, and flexibility in surrounding areas of the body such as the ankle, hip, and spine also can affect the knee. Taking these body regions into consideration is important to help prevent knee OA. Your physical therapist will work with you to help ensure your whole body is moving correctly, as you perform your daily activities.
Real Life Experiences
Luke is a 50-year-old businessman who has just moved his family to the city so he can start a new job. For the last 2 months, Luke has been working hard to fix up his family’s new home, carrying heavy boxes and moving furniture up and down stairs. He also has worked late into the night installing appliances.
After starting his new job last week, sitting through numerous orientation sessions and meetings, Luke notices that his right knee is really hurting. He is used to occasional knee discomfort, but this is the worst it has felt in a long time. During his junior year at college, Luke suffered a significant knee injury while playing basketball, which required surgery.
These days, Luke coaches his son’s Little League team, exercises several times each week, and plays pickup basketball with his friends. But occasionally, particularly after long road trips, his knee pain flares up, and he has to resort to medication, icing, and rest. These bouts are starting to occur more regularly. Luke decides it's time to seek a consultation with a physical therapist.
During Luke’s first appointment, his physical therapist asks him questions regarding his medical history, prior injuries, current symptoms and complaints, and goals for physical therapy. She examines his knee motion, strength, balance, and walking mechanics. She also uses special tests and measures to determine the nature of Luke’s pain, ruling out any other possible conditions.
Based on her findings, Luke's physical therapist determines that his current knee pain is a result of posttraumatic osteoarthritis. She diagnoses knee OA. She explains that his history of significant knee injury in college put him at risk of developing knee OA at a young age. The recent increased demand on his knee joint during his move is likely responsible for the current flare-up of pain and swelling.
Over the next 6 weeks, Luke works with his physical therapist to decrease his joint pain and improve his knee motion and full-body flexibility. She uses manual therapy techniques to improve the mobility of his knee joint. She prescribes a progressive exercise program to strengthen the muscles of his hip, knee, and core. She tailors this program so that Luke can complete it daily, based on the equipment available at his office gym facility.
Six weeks later, Luke is able to climb and descend stairs, squat, and jog without pain. He can sit through a full day of meetings without noticing stiffness or swelling in his knee. On his last day of therapy, Luke’s physical therapist provides him with a detailed home-exercise program and suggestions for maintaining the improvements he has made. With the summer approaching, he's preparing to coach his son's baseball tournaments—and take his family to the beach!
This story was based on a real-life case. Your case may be different. Your physical therapist will tailor a treatment program to your specific case.
What Kind of Physical Therapist Do I Need?
All physical therapists are prepared through education and clinical experience to treat a variety of conditions or injuries. You may want to consider:
A physical therapist who is experienced in treating people with knee osteoarthritis and after knee replacement surgery. Some physical therapists have a practice with an orthopedic focus.
A physical therapist who is a board-certified orthopedic clinical specialist. This physical therapist will have advanced knowledge, experience, and skills that may apply to your condition.
You can find physical therapists who have these and other credentials by using Find a PT, the online tool built by the American Physical Therapy Association to help you search for physical therapists with specific clinical expertise in your geographic area.
General tips when you're looking for a physical therapist (or any other health care provider):
Get recommendations from family and friends or from other health care providers.
When you contact a physical therapy clinic for an appointment, ask about the physical therapists' experience in helping people with arthritis.
During your first visit with the physical therapist, be prepared to describe your symptoms in as much detail as possible, and report activities that make your symptoms worse.
Further Reading
The American Physical Therapy Association (APTA) believes that consumers should have access to information that could help them make health care decisions and also prepare them for their visit with their health care provider.
The following articles provide some of the best scientific evidence related to physical therapy treatment of arthritis. The articles report recent research and give an overview of the standards of practice both in the United States and internationally. The article titles are linked either to a PubMed* abstract of the article or to free full-text, so that you can read it or print out a copy to bring with you to your health care provider.
Brosseau L, Taki J, Desjardins B, et al. The Ottawa panel clinical practice guidelines for the management of knee osteoarthritis; part two: strengthening exercise programs. Clin Rehabil. 2017;31:596–611. Article Summary in PubMed.
Deshpande BR, Katz JN, Solomon DH, et al. Number of persons with symptomatic knee osteoarthritis in the US: impact of race and ethnicity, age, sex, and obesity. Arthritis Care Res (Hoboken). 2016;68:1743–1750. Article Summary in PubMed.
Ackerman IN, Bucknill A, Page RS, et al. The substantial personal burden experienced by younger people with hip or knee osteoarthritis. Osteoarthritis Cartilage. 2015;23:1276–1284. Article Summary in PubMed.
Katz JN, Brophy RH, Chaisson CE, et al. Surgery versus physical therapy for a meniscal tear and osteoarthritis [published correction appears in: N Engl J Med. 2013;369:683]. N Engl J Med. 2013;368:1675–1684. Free Article.
Segal NA. Bracing and orthoses: a review of efficacy and mechanical effects for tibiofemoral osteoarthritis. PM R. 2012;4(5 Suppl):S89–S96. Article Summary on PubMed.
Jansen MJ, Viechtbauer W, Lenssen AF, et al. Strength training alone, exercise therapy alone, and exercise therapy with passive manual mobilisation each reduce pain and disability in people with knee osteoarthritis: a systematic review. J Physiother. 2011;57:11–20. Free Article.
Bennell KL, Hinman RS. A review of the clinical evidence for exercise in osteoarthritis of the hip and knee. J Sci Med Sport. 2011;14:4–9. Article Summary on PubMed.
Lawrence RC, Felson DT, Helmick CG, et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States, part II. Arthritis Rheum. 2008;58:26–35. Free Article.
* PubMed is a free online resource developed by the National Center for Biotechnology Information (NCBI). PubMed contains millions of citations to biomedical literature, including citations in the National Library of Medicine’s MEDLINE database.
Authored by Laura Stanley, PT, DPT, Board-Certified Clinical Specialist in Sports Physical Therapy. Reviewed by the MoveForwardPT.com editorial board.